

Weekly meetings at the Leslie Simon Breast Care and Cytodiagnosis Center formulate treatment plans with the benefit of many opinions
Many women are told by their physicians to get screened for breast cancer; however, exactly when that screening should start has become a topic of disagreement.
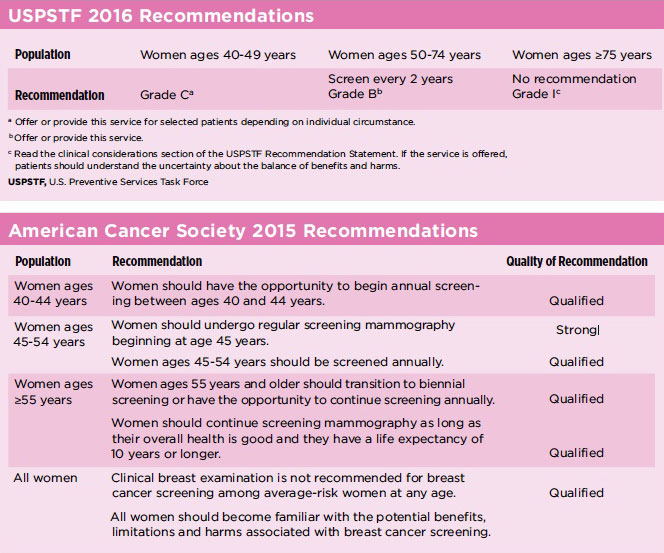
 Several organizations have published guidelines for breast cancer screening in the past two years, including the U.S. Preventive Services Task Force (USPSTF) and the American Cancer Society (ACS). Both organizations have established screening guidelines written by internists and oncologists, but they differ slightly.
Several organizations have published guidelines for breast cancer screening in the past two years, including the U.S. Preventive Services Task Force (USPSTF) and the American Cancer Society (ACS). Both organizations have established screening guidelines written by internists and oncologists, but they differ slightly.
The USPSTF recommends women undergo biennial mammography starting at 40 to 50 years of age. The ACS, on the other hand, recommends women of average risk have screening exams from ages 40 to 44, and annual mammography from 45 to 54. From age 55 onward, women should undergo mammography every other year, although continuing annual screening is acceptable.
Although the traditional U.S. guidelines recommend annual screening beginning at age 40, countries such as the United Kingdom and Canada require screening later and less frequently. With that in mind, physicians at Englewood Hospital and Medical Center examined the issue to determine how early and how frequently breast cancer screening should take place.

“We looked at a comprehensive set of data over many years and found that if we followed less stringent guidelines, we would have missed 20% of all breast cancer cases,” said Miguel Sanchez, MD, chief of pathology at Englewood Hospital and medical director of the Leslie Simon Breast Care and Cytodiagnosis Center. “That’s a substantial number that would have slipped under the radar.”
The data are compelling for physicians at the breast center, which has over 55,000 patient visits per year. “We’re seeing that many patients, and we still don’t recommend loosening the screening guidelines,” Dr. Sanchez said. “It’s something we discuss in our weekly conference and really dissect how changes will affect our detection rate.”

The ACS’s current guidelines have received criticism for the high number of false-positive results that mammograms produce, as well as the detection of noninvasive stage 0 cancers that lead to aggressive treatments. “We are able to provide our patients with mammogram results while they wait. So if additional imaging is needed, it can be performed during the same visit. As a result, our patients do not have to be anxious about false-positive results,” said Mindy Goldfischer, MD, chief of breast imaging at Englewood Hospital.
“At present, we cannot tell which breast cancers will remain stage 0 and which will become invasive. In the near future, ongoing research will likely be able to provide individualized treatment recommendations based on a person’s specific tumor type,” Dr. Goldfischer said.
The physicians at Englewood Hospital rely on science, their expertise and a spirit of collaboration imbued in the center’s professional culture to determine the best care for their patients. “Guidelines are simply guidelines, but not necessarily what a physician must follow,” said Violet Merle McIntosh, MD, section chief of breast surgery at Englewood Hospital. “We look at the individual and ask, ‘Does the patient have reasons to be screened more closely? Is there something about the woman’s family history? Does her race or genetic history suggest we should screen earlier?'”
Dr. McIntosh believes women identified as high risk should have a baseline screening at age 35, a second screening around age 38 and an annual screening starting at age 40. “While low-risk women could wait until 40, the notion of waiting until 50 is not sensible,” she said. “Seventypercent or more of breast cancer cases we see are from women with no family history of breast cancer. So it really doesn’t make sense to wait to screen just because you don’t know of breast cancer in the last few generations. “And with the increasing use of 3-D mammograms, the false-positive rate has decreased,” Dr. McIntosh said. “Primary care physicians are encouraged to continue referring patients for screening.”
Physicians at Englewood Hospital meet every Wednesday with the oncologists, surgeons, geneticists, pathologists, radiologists and radiation oncologists to discuss every new patient case and to create an individual plan for each patient. The meeting is broadcast live to international hospitals trying to emulate Englewood’s program.
These weekly meetings address more than just how to treat a tumor. “We present the patient’s history, images and pathology,” Dr. Goldfischer said. “We address social issues such as, ‘How will an elderly woman living alone get to the hospital for daily radiation treatments?’ All aspects of the individual patient’s medical and social history are considered when we formulate a treatment plan.”
“Our weekly multidisciplinary conference is unique,” Dr. Sanchez said. “It is composed of physicians of every subspecialty related to the diagnosis and treatment of breast cancer, in addition to the patient navigator, nurse practitioner who specializes in genetics, nurse who runs clinical trials, social worker, residents and tumor registrar. And for the patient, you don’t get one second opinion—you may get many second opinions.”
Posted March 2017
Weekly meetings at the Leslie Simon Breast Care and Cytodiagnosis Center formulate treatment plans with the benefit of many opinions